
Cervicogenic dizziness & Sensorimotor Dysfunction
Dizziness accounts for approximately 5% of presentations in primary care (Susanto, 2014). It has been reported to be present in up to 24% of patients with cervicogenic headache (Sjaastad & Bakketeig, 2008) and 75% in patients with chronic whiplash and associated disorders (WAD) (Treleaven et al., 2008).
Dizziness can be categorised by the cause of dizziness:
- Cardiac,
- Psychological,
- Medication induced,
- Vestibular,
- Metobolic,
- Neutrally-mediated, and
- Cervicogenic.
So what is cervicogenic dizziness? Similar to the term cervicogenic headache, cervicogenic dizziness is a symptom of dizziness, unsteadiness or light-headedness, that is thought to originate from dysfunction within the cervical spine. Cervicogenic dizziness is a non-specific symptom of altered orientation in space and disequilibrium and is differentiated from specific causes of dizziness such as vertigo and vertebra-basilar artery insufficiency (Treleaven, Jull, & Sterling, 2003).
Normal sensorimotor function is a result of collaborative inputs from the visual, vestibular and postural-control systems. As such, disturbance in sensorimotor function can be a result of disruption in any/all of these systems (Dispenza, De Stefano, Mathur, Croce, & Gallina, 2011; Sterling, Falla, Jull, Treleaven, & O'Leary, 2008).
“Impairments in sensorimotor features such as eye movement control, cervical joint position sense and postural stability, affecting balance have been found in association with persistent neck pain of both insidious and traumatic origins” (Treleaven, Clamaron Cheers, & Jull, 2011, p. 636). Cervicogenic dizziness can occur in both traumatic and non-traumatic cases.
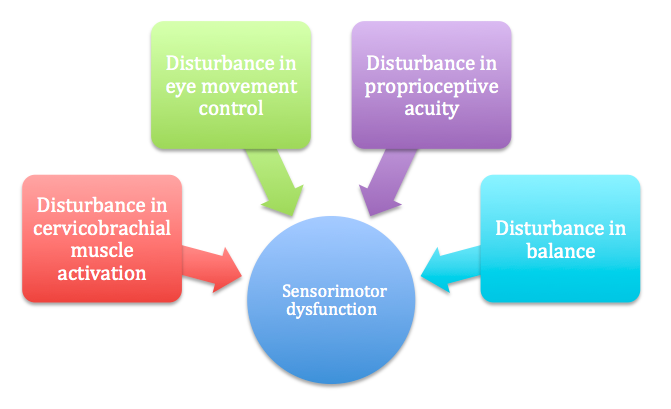
Multiple variables that contribute to the development of sensorimotor dysfunction.
WHAT ARE THE NEURO-PHYSIOLOGICAL MECHANISMS OF CERVICOGENIC DIZZINESS, LIGHT-HEADEDNESS & UNSTEADINESS?
The cervical spine contributes to somatosensory awareness via the following mechanisms (Sterling, et al., 2008; Treleaven, et al., 2011):
MECHANORECEPTORS:
Cervical spine mechanoreceptors found in the muscle spindles, joints and ligaments are found in high density in the upper cervical spine. Especially in the sub-occipital and upper cervical spine muscles, there are high numbers of muscle spindle mechanoreceptors that play a large role in sensorimotor function and proprioceptive sense. These cervical afferents provide proprioceptive sense by feeding information to the central nervous system through the ventral and dorsal horns in the spinal cord. Once the messages enter the spinal cord they can then travel up the spinothalamic, spinocerebellar and propriospinal tracts to central nervous system structures such as the thalamus, cerebellum and somatosensory cortex.
REFLEXES:
Cervical afferents also help to mediate messages and reflexes from the vestibular and visual systems with direct input to the medial and lateral vestibular nuclei, the dorsal column nuclei, central cervical nuclei, and superior colliculus.
SYMPATHETIC NERVOUS SYSTEM:
Cervical afferents may also communicate with the sympathetic nervous system through beta-receptors in the muscle tissues and these pathway is bi-direction.
Why do cervical receptors have such a wide network of connections? The reason being that cervical receptors play a role in neck reflex activity relating to “head orientation, eye movement control and postural stability” (Sterling, et al., 2008, p. 62). That is to say they have a crucial role in proprioception, posture, spatial awareness and coordination of eye movements (Treleaven, et al., 2005).
WHAT REFLEXES ARE INVOLVED IN SENSORIMOTOR FUNCTION?
Visual acuity:
Visual acuity is controlled by the Cervico-occular reflex (COR) and the Vestibulo-occular reflex (VOR). These two reflexes COR and VOR help to coordinate extra-occular muscles which ensure eye movements are equal and opposite to head movements to allow for clear vision.
Vestibulo-occular reflex (VOR):
- Stabilises images on the retina during head movement to ensure visual acuity.
- Sends information to the CNS which then creates a motor output to control movement of the eyes.
- The VOR is often assessed with the Head-thrust test (when the patient fixates gaze on a target and rotates the head from side to side).



Cervico-occular reflex (COR) :
- The COR is an afferent input from muscles in the neck.
- This is often assessed with the Smooth Pursuit Neck Torsion test (SPNT) where the patient holds their head still and gaze fixed and the trunk is rotated from side to side (to activate muscles in the neck).
Postural stability:
Tonic neck reflex (TNR) is activated by muscles in the neck and works to activate muscles in the limbs to create stable posture and steady base of support for balance. It also integrates with the vestibulospinal reflex in activating spinal muscles used in postural stability. This tonic neck reflex is only assessable in infants and appears with ipsilateral arm flexion and contralateral arm extension with neck rotation. This reflex is not seen in a mature neurological system (Brandt & Bronstein, 2001).



Instead we assess overall balance and postural control with tests such as the Rhomberg's test or Balance Error Scoring System (BESS) to evaluate vestibular, visual, and proprioceptive contributions to balance.
Maintenance of head position:
The cervicocollic reflex (CCR) works with the vestibulocollic reflex (VCR) to maintain head position. The CCR relies on information from muscle spindle (mostly) and joint receptors activity when muscles are stretched with movement. Sterling, et al. (2008) suggest that this information is derived from the rectus capitus posterior major, obliquus capitus inferior and the splenius muscles.
HOW DO CERVICAL AFFERENT MESSAGES BECOME DYSFUNCTIONAL?
As you can see from the information above, the cervical spine has a strong influence on the maintenance of head position and connection to postural stability and visual acuity. Thus, dysfunctional afferent messages from the cervical spine can be responsible in disruption of sensorimotor control.
- This can occur as a result of direct trauma (e.g. whiplash or injury) or from alterations in afferent feedback due to incorrect muscular function.
- The cervical spine afferents are susceptible to chemical neural irritation from local inflammatory mediations in the surrounding tissues.
- Such dysfunction may also occur in the presence of nociception there may be a direct effect from centrally driven mediators.
- And finally, the sympathetic nervous system may exert an effect on the muscle spindle activity resulting in alterations in muscle activity.
In summary
The cervical spine plays a large role in normal sensorimotor function. Disruption in sensorimotor control may result in a sensation of disequilibrium. If the cervical spine is the primary contributor to this disequilibrium, then it can be concluded (following exclusion of other sources of dizziness) that the patient has cervicogenic dizziness.
The mechanisms for such symptoms have been outlined above. The next questions to answer are what are the symptoms of cervicogenic dizziness and how can they be distinguished from other causes of dizziness? To answer these questions, we must first look at the symptomology of dizziness and physical examination. You will need to draw the descriptors out of the patient during the subjective examination and in order to do that, you need to specifically word the questions you ask. The next blog will explore the differential diagnosis of dizziness and also assessment of the vestibular system, occulo-motor system, cervical spine and balance.
Sian
References:
Brandt, T., & Bronstein, A. M. (2001). NOSOLOGICAL ENTITIES?: Cervical vertigo. Journal of neurology, neurosurgery and psychiatry, 71(1), 8‐12.
Cherchi, M. (2011). Infrequent causes of disequilibrium in the adult. Otolaryngologic clinics of North America, 44(2), 405‐414, ix.
Dispenza, F., De Stefano, A., Mathur, N., Croce, A., & Gallina, S. (2011). Benign paroxysmal positional vertigo following whiplash injury: a myth or a reality? American journal of otolaryngology, 32(5), 376-380.
Halmagyi, G. M., & Halmagyi. (2000). Assessment and treatment of dizziness. Journal of neurology, neurosurgery and psychiatry, 68(2), 129‐134.
Moubayed, S. P., & Saliba, I. (2009). Vertebrobasilar insufficiency presenting as isolated positional vertigo or dizziness: A double‐blind retrospective cohort study. The Laryngoscope, 119(10), 2071-2076.
Schenk, R., Coons, L. B., Bennett, S. E., & Huijbregts, P. A. (2006). Cervicogenic dizziness: A case report illustrating orthopaedic manual and vestibular physical therapy comanagement. The Journal of manual & manipulative therapy, 14(3), E56‐E68.
Sjaastad, O., & Bakketeig, L. S. (2008). Prevalence of cervicogenic headache: Vaga study of headache epidemiology. Acta neurologica Scandinavica, 117(3), 173-180.
Sterling, M., Falla, D., Jull, G., Treleaven, J., & O'Leary, S. (2008). Whiplash, headache, and neck pain: research-based directions for physical therapies: Elsevier Health Sciences.
Susanto, M. (2014). Dizziness: if not vertigo could it be cardiac disease? Australian family physician, 43(5), 264.
Treleaven, J., Clamaron Cheers, C., & Jull, G. (2011). Does the region of pain influence the presence of sensorimotor disturbances in neck pain disorders? Manual therapy, 16(6), 636-640.
Treleaven, J., Jull, G., & Low Choy, N. (2004). Smooth pursuit neck torsion test in whiplash-‐associated disorders: relationship to self-‐reports of neck pain and disability, dizziness and anxiety. Journal of rehabilitation medicine, 37(4), 1‐1.
Treleaven, J., Jull, G., & Low Choy, N. (2005). Standing balance in persistent whiplash: a comparison between subjects with and without dizziness. Journal of rehabilitation medicine, 37(4), 224-229.
Treleaven, J., Jull, G., & Sterling, M. (2003). Dizziness and unsteadiness following whiplash injury: characteristic features and relationship with cervical joint position error. Journal of rehabilitation medicine, 35(1), 36‐43.
Treleaven, J., LowChoy, N., Darnell, R., Panizza, B., Brown-Rothwell, D., & Jull, G. (2008). Comparison of sensorimotor disturbance between subjects with persistent whiplash-associated disorder and subjects with vestibular pathology associated with acoustic neuroma. Archives of Physical Medicine and Rehabilitation, 89(3), 522-530.